The extraocular muscles are the powerhouse of eye movement. They work behind the scenes, shifting our gaze, tracking objects, and keeping vision stable as we move through the world. Six muscles1 control these precise movements, each playing a vital role in positioning the eyes. Whether looking up, down, side to side, or adjusting for fine movements, these muscles respond instantly, ensuring seamless coordination.
Optometrists rely on a deep understanding of extraocular muscles to assess eye function. Weakness, imbalance, or nerve-related issues can disrupt their smooth operation, leading to symptoms like double vision, abnormal head positioning, or difficulty focusing. Recognising how they interact is key to identifying motility disorders2 and guiding clinical decisions.
This article breaks down each extraocular muscle, explaining its function, the way it moves the eyes, and why its role matters in everyday vision. By the end, you’ll feel more confident in the extraocular muscles and what they do. Be sure to check out the other articles in the Binocular Vision section of the Skill Centre for further information.
The Six Extraocular Muscles and Their Actions
The extraocular muscles keep your eyes in motion, shifting them effortlessly in all directions. Each eye relies on six muscles1 working in coordination, ensuring smooth, controlled movements for tracking, focus changes, and gaze stability.
The Rectus Muscles: Straight Movers
These four muscles originate from the Annulus of Zinn3, a fibrous ring at the back of the orbit. They extend forward, attaching to the front half of the sclera to pull the eye in a straight line.
- Medial Rectus (Innervated by CN III – Oculomotor2): Moves the eye inward (adduction) towards the nose.
- Lateral Rectus (Innervated by CN VI – Abducens2): Moves the eye outward (abduction) towards the temple.
- Superior Rectus (Innervated by CN III – Oculomotor2): Moves the eye upward (elevation). It also slightly adducts and intorts (rotates inward).
- Inferior Rectus (Innervated by CN III – Oculomotor2): Moves the eye downward (depression) with secondary adduction and extorsion (rotates outward).
The Oblique Muscles: Rotators and Refiners
These muscles adjust eye position subtly, fine-tuning rotation and vertical movements, especially when looking diagonally.
- Superior Oblique (Innervated by CN IV – Trochlear2): Intorts (rotates inward), depresses the eye, and assists in abduction. Its tendon runs through the trochlea, a small pulley that redirects its pull.
- Inferior Oblique (Innervated by CN III – Oculomotor2): Extorts (rotates outward), elevates the eye, and also helps with abduction. It’s the only extraocular muscle that doesn’t originate at the Annulus of Zinn, instead arising from the medial orbital floor.

Together, these muscles work in balanced pairs, while one contracts, its opposite relaxes. This coordination follows Sherrington’s Law, ensuring smooth movement without resistance. Meanwhile, Hering’s Law ensures yoke muscles (pairs of muscles that work together for a specific gaze direction) in each eye receive equal neural signals, keeping both eyes perfectly aligned during movement.
Every glance, every shift in focus depends on these muscles executing precise actions. When something disrupts their function; whether from nerve damage, muscle weakness, or restriction, it affects both sight and comfort. That’s why it is important to assess their function during every eye examination.
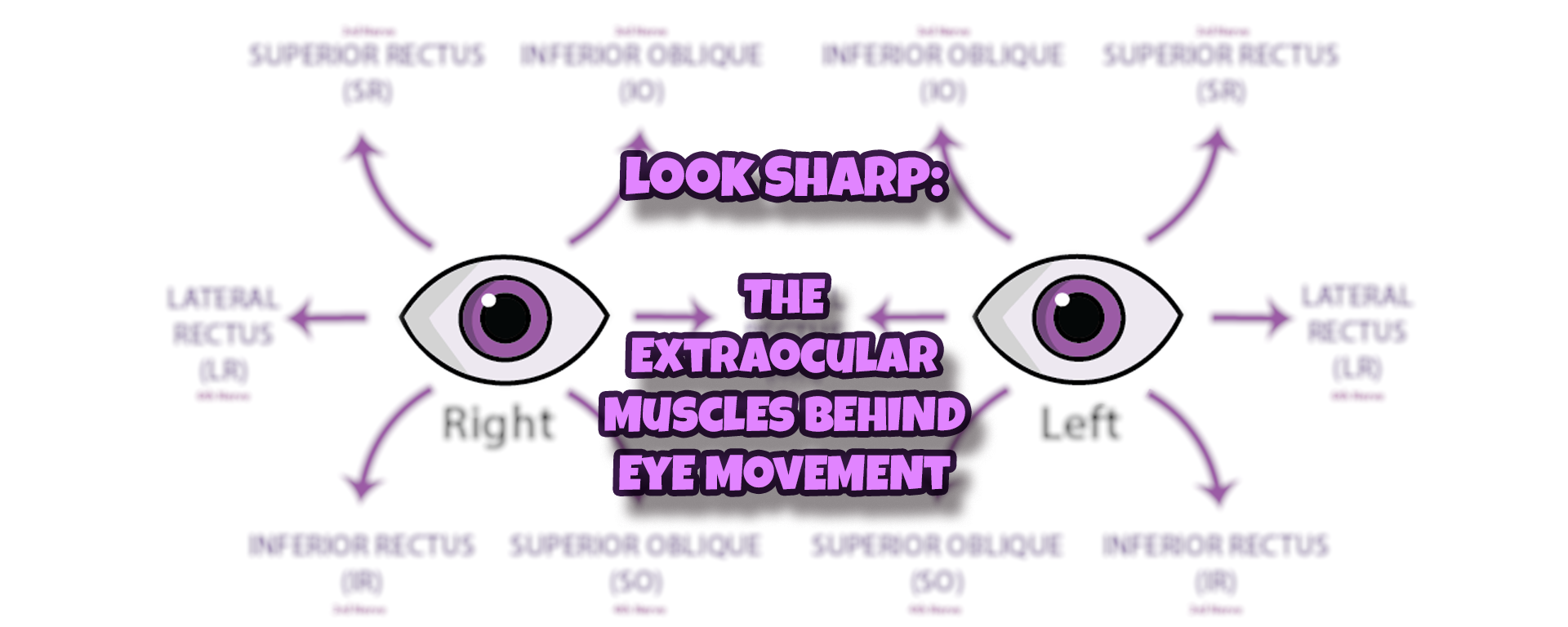
Movements Summarised
The following diagram and table helps to summarise these muscle movements.

| Extraocular Muscle | Primary Action | Secondary Action | Tertiary Action |
| Lateral Rectus | Abduction | ||
| Medial Rectus | Adduction | ||
| Superior Rectus | Elevation | Intorsion | Adduction |
| Inferior Rectus | Depression | Extorsion | Adduction |
| Superior Oblique | Intorsion | Depression | Abduction |
| Inferior Oblique | Extorsion | Elevation | Abduction |
How Extraocular Muscles Work Together
The extraocular muscles don’t act alone – every eye movement relies on precise coordination between muscle pairs. Whether looking left, right, up, or down, each muscle has an opposite counterpart that balances its motion.
Take Sherrington’s Law of Reciprocal Innervation. When a muscle contracts to move the eye in one direction, its antagonist (opposite) relaxes to allow smooth movement4. For example, the lateral rectus moves the eye outward, but only because the medial rectus lets go. The same happens with vertical movements—the superior rectus lifts the eye while the inferior rectus eases off.

Now, for Hering’s Law of Equal Innervation. Synergistic muscles in both eyes receive identical neural signals when moving together5. Look right, and the right lateral rectus pulls the eye outward while the left medial rectus does the same on the other side. Their equal activation keeps both eyes moving in sync, avoiding double vision.

This teamwork is essential for clear sight, depth perception, and comfortable eye movement. Without it, gaze would be jerky or misaligned, leading to strain or diplopia.
Optometrists assess these relationships to diagnose issues like nerve palsies, muscle imbalances, or restrictions from conditions like thyroid eye disease6. By understanding how extraocular muscles coordinate, clinicians can detect movement disorders early and guide treatment effectively.
Why Actions of the Extraocular Muscles Depend on Eye Position
Extraocular muscles don’t work in isolation2,5. Their actions shift depending on where the eye is positioned. A muscle’s primary function might change entirely depending on whether the eye is looking straight ahead or turned to the side.
Take the superior rectus. When the eye is in its neutral position, it lifts the eye upwards. But if the eye is turned inwards, the superior rectus becomes more responsible for intorsion (rotating inward). The same goes for the inferior rectus—when the eye is turned outward, its downward pull is stronger, but when adducted, it mainly extorts the eye.
The oblique muscles work similarly. The superior oblique typically controls intorsion, but when the eye turns inward, it plays a larger role in depression. The inferior oblique, usually an extorter, becomes an elevator when the eye moves inward.
Understanding these shifts is crucial for optometrists. Certain conditions, like cranial nerve palsies, may cause weakness in specific muscles that only show up in certain gaze positions7. That’s why eye movement is assessed in all directions – it reveals underlying issues that might otherwise go unnoticed.
By observing how the extraocular muscles function across different positions, clinicians can pinpoint where something is going wrong7, guiding both diagnosis of which muscle isn’t doing it’s job – and suggest what may be the underlying cause.
Clinical Significance of Extraocular Muscle Function
Extraocular muscles don’t just move the eyes—they help optometrists spot potential issues early. If a muscle isn’t working as expected, it can point to underlying conditions affecting eye movement, nerve function, or overall health.
Cranial nerve palsies are a common concern. A CN III palsy (also referred to as a “third nerve palsy”8) can leave the eye positioned down and out, often with ptosis and a dilated pupil if parasympathetic fibres are affected8. A CN IV (also referred to as a 4th nerve palsy9) palsy may cause vertical double vision, with patients tilting their heads to compensate9. CN VI palsy (known also as 6th nerve palsy10) results in difficulty abducting the eye10, making sideways gaze uncomfortable.

Other conditions, like thyroid eye disease, restrict muscle movement through fibrosis, often affecting elevation. Myasthenia gravis, a neuromuscular disorder, can create fluctuating weakness in eye muscles, causing unpredictable motility changes. Optometrists also assess binocular vision issues, spotting misalignment patterns that impact comfortable sight.
By evaluating how extraocular muscles function, optometrists help identify neurological, mechanical, or systemic conditions that require further investigation. Understanding their role is essential for diagnosing motility disorders and guiding patient care.
Tales from Jason’s Clinic
Some of the most memorable cases in optometry don’t come from textbook scenarios—they unfold in real time, often when least expected.
One stands out from about eight years ago. A gentleman came in for a post-cataract assessment, frustrated by persistent headaches that developed after his pre-cataract appointment. Though the visit was purely for research, something was clearly off. His right eyelid drooped shut, his eye was positioned down and out, and his pupil was blown. Motility wasn’t part of my research protocol, but seeing these signs appear, especially together, they pointed straight to oculomotor nerve dysfunction – a classic red flag for a third nerve palsy. That referral to eye casualty and the neuro-ophthalmologist confirmed the worst: a brain tumour. It was a reminder that even in routine checks, knowledge of ocular motility can pick up life-threatening conditions.
Then there was the patient booked in for me with a suspected chalazion. Most signs and symptoms suggested meibomian gland dysfunction, but the mild lid oedema raised a concern. With extra caution, motility testing was added, and despite her straight-looking eyes, she reported diplopia and discomfort. The signs suggested early orbital cellulitis. That extra step in investigation meant a timely referral, rapid treatment, and full recovery.
Diplopia often disrupts daily life more than people expect. Many patients describe struggling with reading, driving, or even simple visual tasks. A thorough case history is essential in pinpointing risk factors and causes -something I expand on in my book, History and Symptoms: The Eye Examination. You can purchase your copy on Amazon here.

Even when the primary complaint seems straightforward, knowing how the extraocular muscles behave in different conditions can make all the difference in patient care – so do take the time to learn them!
Final Thoughts
Extraocular muscles may not be something most people think about, but they’re working constantly to keep our vision clear, stable, and aligned. Their precise movements allow us to shift focus, track objects, and maintain depth perception without a second thought.
For optometrists, understanding these muscles is essential—not just for identifying eye movement disorders, but for spotting systemic and neurological conditions early. Whether assessing a patient’s motility or recognising signs of nerve dysfunction, a deep knowledge of extraocular muscle function enhances clinical care.
From detecting third nerve palsies to identifying restrictive motility issues, these muscles hold vital clues about a patient’s health. The ability to recognise abnormal movement patterns and their underlying causes can make all the difference in timely diagnosis and management.
In practice, every eye movement tells a story, and knowing how to interpret it ensures the best possible outcomes for patients. A future article will cover how to assess these movements in clinic.
Skill Activity
Extraocular Muscles Skill Activity
Further Reading
The following resources were used in creating this article on the extraocular muscles.
- Spencer RF, and Porter JD (2006). Biological organization of the extraocular muscles. Progress in Brain Research 151: 43-80.
- Haladaj R (2019). Normal anatomy and anomalies of the rectus extraocular muscles in human: a review of the recent data and findings. Biomed Research International 2019. [Online.] Available at: https://onlinelibrary.wiley.com/doi/full/10.1155/2019/8909162 [Accessed: May 4th 2025].
- Ansari MW, and Nadeem A (2016). Extraocular and Intraocular Muscles. In: Atlas of Ocular Anatomy. Springer, Cham. pp 39-51.
- Sherrington CS (1905). On reciprocal innervation of antagonistic muscles.―Eighth note. Proceedings of the Royal Society B 76(509). 269-297.
- Moschovakis AK, Scudder CA, and Highstein SM (1990). A structural basis for Hering’s Law: projections to extraocular motoneurons. Science 248(4959): 1118-1119.
- Scott IU, and Siatkowski RM (2009). Thyroid eye disease. Seminars in Ophthalmology 14(2): 52-61.
- Gold D (2021). Motility and ocular motor disorders. In: Neuro-Ophthalmology and Neuro-Otology. Springer, Cham. pp 125-190. Available at: https://link.springer.com/chapter/10.1007/978-3-030-76875-1_4#citeas [Accessed: May 4th 2025].
- Keane JR (2010). Third nerve palsy: an analysis of 1400 personally-examined inpatients. Canadian Journal of Neurological Science 37: 662-670.
- Keane JR (1993). Fourth nerve palsy: historical review and study of 215 inpatients. Neurology 43(12): 2439.
- Peters III GB, Bakri SJ, and Krohel GB (2002). Cause and prognosis of nontraumatic sixth nerve palsies in young adults. Ophthalmology 109(10): 1925-1928.
Leave a Reply